PRESENTATION HIGHLIGHTS
On how the Institute for Stem Cell and Regenerative Medicine (ISCRM) pivoted to tackle COVID-19 head on
Dr. Chuck Murry: ISCRM is the largest interdisciplinary research unit at the University of Washington with members of 37 different departments in the College of Arts and Sciences, the College of Engineering and the School of Medicine; as well as, Fred Hutchinson Cancer Center, Seattle Children’s and other private institutes around Seattle.
Our mission really is to harness the power of stem cells to create new medicines for today’s patients.
So, when COVID happened, it was clear that we were going to have to have a major shutdown of most of the research facilities. But some of our teams decided to pivot the research that was going on in their laboratories and tackle this disease head-on.
COVID affects the lungs. But we’re learning it’s not just the lungs, that there’s many organs in the body that get impacted by this particular coronavirus. Because we can grow most of the cells of the human body now through stem cells, we’ve been studying the impact that COVID has not just on the lungs but on the heart, the kidney and the brain as well.
On using robots to test thousands of possible COVID-19 therapies
Dr. Chuck Murry: One of the things we wanted to do was take our robots that do high-throughput screening, to do this we had to create a bubble within the containment facility, and our robots live inside of this little biosafety containment enclosure that we had to purchase. Using miniaturized systems with rapidly liquid-transferring robots, we can do lots more experiments than could ever be done with human hands.
Our goal is basically to find new drugs that inhibit this virus from entering the cell, that block the virus from replicating, key stages in its life cycle. And we got our first set of data just two days ago. [Editor’s note: this recording was made on July 30, 2020.] And so we set up lung cells in these little miniature test tubes. And then we take these lung cells and we give them just enough coronavirus so that over a 48-hour period, half of them are going to die. And that lets us see whether the drugs we add make things better or make things worse.
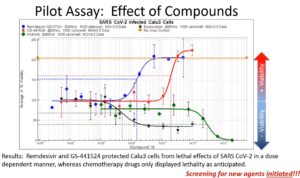
And so in this particular data plot , when things go up, that means the cells are happy and healthy, and when things go down, that means they’re dying. So we used two drugs that we knew would make cells die. These are cancer-chemotherapy drugs. And both of these cancer drugs, as expected, kill off the lung cells.
But two drugs actually bring viability up to essentially 100%. And it turns out that this one that was the most potent is one that you’ve already heard of. That’s called remdesivir. This is the compound from Gilead pharmaceuticals that’s had a major impact on shortening the hospital stays for patients who have severe COVID-19 infection. So that tells us that this assay is working.
And what we’re doing now is testing every drug that the FDA has ever approved. This is about 2,500 drugs or so. And we will screen all of these first, because there’s nothing faster than repurposing an already existing drug.
And after that, we’ll go one step back, everything that was safe but maybe not so effective in earlier trials for other diseases, and so forth. And so we plan to screen many tens of thousands of drugs and drug-like molecules and endeavor to find new treatments for this disease. So that’s just one way that the Institute is engaging in this fight against COVID-19.
On sending heart cells on SPACE X
Dr. Nate Sniadecki: For the last two years, we’ve had a team of engineers, biologists, cardiologists working together to send a package 240 miles up to the International Space Station with 48 little engineered heart tissues made from stem cells.
But you know, I missed the Space X flight. I wasn’t there for the launch, but the package did make it. So why were we doing this? Why were we sending these heart tissues up to the space station? Well, when you’re in space, you miss the effects of gravity, and astronauts, there’s not much space in space. They live in a confined environment. The lack of gravity changes how the blood flows in their body.
Normally, gravity holds a lot of blood down by your legs and feet. But when you’re in space, the blood pressure equalizes everywhere. And so you get this kind of puffy face reaction as the blood rushes to your head. And it causes a lot of problems with your heart. Astronauts that spend a long time in space, they lose heart mass, and the heart doesn’t work as well from this long-term travel.
But also, being able to do better research on human heart tissue, you can’t really do that with a lot of humans up in space. So instead of sending more and more astronauts, the goal really was to see if our engineered heart tissues could be affected by microgravity in some similar way as the hearts of astronauts. So we had taken what we had developed on earth to send it up to the space station for a four-week visit.
On engineered heart tissue

Dr. Nate Sniadecki: Well, these are made from stem cells, and we can turn them into new heart muscle, or cardiomyocytes. So, what you’re seeing here is an array of pillars with little heart strings attached to each pair of pillars. And those strings are a three-dimensional heart tissue. There’s about 500,000 heart cells in those tissues. They live in a 3D world, which is more like what you would have in the human body. So these cells look more like you would see from real human heart tissue. The structure matches. The density matches very nicely. And because they’re suspended between these pillars, we can measure how strong they are. These tissues contract.
If you look carefully, you’ll see these little red squares in each of the pillars. Those are little magnets. And that actually allowed us to do some amazing measurements up on the space station. What those little magnets are doing is they’re working with an effect called the giant magnetoresistance.
What this does is, when there’s a change in the magnetic field, it changes the resistance in a thin film. And so you can get a voltage reading this way. So with those engineered heart tissues, every time they contract, they move the position of that magnet. And we can pick up that change in the magnetic field through a voltage reading. So just by using some printed circuit boards underneath the chambers, we can electrically listen to the heartbeats.
And so we can do this remotely. We don’t need to have a microscope. We don’t need to send a microscope up to the space station. And we can do it in real time So we can actually get data back from the space station 240 miles away.
We have all these different heartbeats of these tissues over time. And so, if you add a beta blocker like verapamil, you actually see the heartbeat stop. Or if you add something like adrenaline or isoproterenol, you actually see an increase in the beating frequency when you add that drug.
There was a bit of an Apollo 13 moment for us in this work. The team down in Florida left, actually, in February before things went really bad. So they made it down, but I didn’t get to go. But Jonathan and Ty really kind of pulled a late-night preparation effort, because things weren’t quite working the way we wanted to. And they watched from a distance as our package went up to space, and we were fingers crossed, hoping that all of our equipment would survive the rocket launch.
On the heartbeat in space
Dr. Nate Sniadecki: We waited kind of on pins and needles for two days until we got our first data. The data we got was quite amazing.
So, over time, we started seeing a detrimental effect, that the effect of microgravity was causing these tissues to get weaker and weaker. So we are really excited about these results because it matches with what a lot of astronauts suffer from. Not only do we see the tissues getting weaker, we start to see slower heartbeats in these tissues, and also more irregular heartbeats, too.
Now, we have to do similar experiments on Earth, but right now we’re delayed because of COVID on that. But you know, when they say, one door closes, another door opens, this is where we took a pivot towards COVID-19. And this really is just the fact that, hey, let’s use everything we can to try to understand what’s going on with this disease.
On understanding COVID-19’s impact on the heart
Dr. Nate Sniadecki: There have been some reports that the coronavirus can also cause injury to the heart. And it’s not quite clear how this is happening.
This is really where Michael Gale, Chuck and I are working to understand this. So, there’s a couple of ways that this could be happening. It could be because the heart is getting damaged from the intense inflammation that’s happening due to the disease. There’s also been reports about blood clots happening from COVID patients, and that could be causing damage to the heart. But more recently, there’s been some evidence about direct viral infection, that the heart itself can become infected by the virus, but it hasn’t yet been proven. And this is really where we’re working to understand if this is possible. So using the same kind of tissues, the same kind of stem cells that we have at UW, we want to understand if this actually is possible.
So how does the virus infect the cells? Well, on the surface of your lung cells, on your blood vessels, your airways and your heart, there’s a protein called the ACE2 receptor. And this is usually involved in helping to regulate your blood pressure. But this is the docking site. This is where the coronavirus can bind like VELCRO to the surface of these cells. It does so through its spike protein. And once it’s stuck on the surface of a cell, it’s able to then enter. It has its RNA become … It hijacks the machinery of the cell to start replicating the virus. And, you know, the fact that the heart tissue can actually express this receptor gives us an indication that it’s likely that this is a way that the heart can be injured by the virus.
So, very early on, we saw that these heart cells can become infected by the virus. The virus can cause these cells to stop beating, and then die. So this is very interesting. We also started working with our engineered heart tissues with the same magnetic-sensing platform that we built for space.
And what we found was quite astounding to us, because we’re actually seeing the virus causing these cells to lose strength over time. And this is data that just came to us today. [Editor’s note: this recording was made on July 30, 2020.] And we’re going to look even further into this to see, is it causing irregular heartbeats in these tissues? What’s really happening to the function of these hearts due to the virus?
This is just one of the examples of using what we’ve developed for space to help us in this battle with COVID.
On the long-term effects of COVID on the heart
Dr. Chuck Murry: This is the first demonstration that the heart is a direct target of COVID-19, and that is super important to know. Because we didn’t know whether this was bystander injury or a direct target. And now we know that the heart is a direct target. The number one cause of death with COVID infection is the failure of the lungs, but probably number two cause is failure of the heart. And so now we know that in maybe 30 to 40% of people who die from COVID, it’s potentially due to this infection of the heart. And once you get informed on something like this, then you can be prepared to respond.
There’s data that’s coming out now that says that patients who have a bad hit of COVID can end up with significant structural heart disease afterwards, and so that people who … when they do cardiac magnetic resonance imaging scans and things like that after somebody’s had a COVID infection, they see sort of diffuse multifocal scarring in their hearts. We hope this will teach us about how to stop its infection, and maybe, down the road, what some of the long-term sequela are.
On how ISCRM was able to pivot so quickly and the roadblocks to doing so
Dr. Chuck Murry: One of the things we found is that, just simply, if you’re going to work with a live virus, this is a slow business. When I said we’re going to pivot, and a chunk of my lab is now going to focus on COVID, I had no idea what I was talking about. I didn’t realize that these very sparsely equipped laboratories wouldn’t be able to do all the kinds of things that I was used to doing in the outside world. I didn’t realize that every time we wanted to bring a simple slide out to look at under a microscope, we would have to go through all these biosafety protocols to prove that we weren’t bringing virus out and that sort of thing. So just the logistics, I had no clue about what the logistics were to work in a facility like that.
What enabled us to pivot quickly was the fact that we had discretionary money. That we didn’t have to write a grant to the federal government and wait for six to 12 months for approval. We could just think of an experiment today, and literally we began doing the work necessary to get going within a day or two. And so that’s extremely nimble. And that’s where philanthropy comes in, that it allows us to do these kinds of super important works while turning on a dime. And so we’re so grateful to the people who’ve supported the institute over the time, over the many years of its existence, because we used donor monies to fund basically all the work that you heard about here.